
S
ince DuQuan Myers died six years ago, he’s come back in ways that are mysterious and magical and hard to explain. It started the day of his funeral, when the doves that were released over his coffin refused to fly home, perching instead in the oak tree just above his grave as if witnessing a visitation. Then there was that drive to El Paso, Texas, when — not once but twice — the windshield wipers started swiping just as the satellite radio cut out midsong, switching to the tune Myers’ sister Natasha had been listening to at the exact moment when her mom called with the news that her brother was gone. There was the way Myers’ nephew — the one who was just a baby when Myers died — would sometimes point into an empty corner of a room and say “uncle.” There were the Pokémon cards that Myers had loved as a child but hadn’t played with in years turning up one by one in unexpected and impossible places, like the middle of a clean kitchen floor. There were the nights when Myers’ mother, Letitia Wilbourn, would feel him, actually feel him, resting his head upon her shoulder, even though no one was there. But, of course, that’s not right. There was someone there. He was there. She knew it. Such is the logic of grief.
Tragedy rips the grieving out of the storyline of their own life, denies them any sense of what the past meant or the future will hold. Wilbourn remembers few details from her son’s funeral, but she does remember the doves. “That lady said, ‘These birds have never done this. Never,’” she tells me, sitting on a small sofa in the darkened living room of her modest house in the suburbs of Fort Worth, surrounded by pictures and mementos from her son’s short life: an infant footprint from the hospital where he was born, a class project he wrote about wanting to own a whale, a photo of him posing in his Little League uniform with a shy smile. “The lady was like, ‘Was he a very gentle spirit?’”
DuQuan Myers was a gentle spirit. His family called him the “animal whisperer,” the kid who loved to roam the farmland that still abutted their Echo Heights neighborhood and who would bring home all kinds of creatures he’d “rescued” — dogs, cats, turtles, frogs, lizards, toads, even once a snake that Wilbourn found, to her horror, in a candy jar. When his three older sisters squabbled, Myers was the one who always could diffuse the situation, the baby brother whose humor and charisma and cheerfulness were impossible to resist. It fit no known narrative that Myers would hurt any living thing, himself included. And yet on the evening of Feb. 17, 2017, Wilbourn had been driving home from her job as a cop for the Tarrant County Sheriff’s Office when she received a phone call. On the other end, she could hear the keening sobs of the young woman Myers had dated off and on for years. “She said, ‘Quan’s dead,’” Wilbourn explains. “I was like, ‘What?’ She said, ‘DuQuan’s dead.’” Home alone in his apartment near Texas State, 26 years old and only months away from getting a degree in criminal justice, Myers had shot himself in the head.
Without thinking, wild with grief, Wilbourn turned her car toward San Marcos and drove 77 miles in 30 blind minutes before a friend called and persuaded her to pull over and turn around. Myers was gone. There was nothing to be done that night, which Wilbourn spent at home, alone, her phone switched off so nothing could puncture the cocoon of mourning and confusion. She’d spoken to Myers earlier that day, just before he’d begun his shift at FedEx. He’d seemed fine, his normal self. But had she missed something? She knew he had a gun, but he lived in Texas; everyone has one. She’d only discussed suicide with him once before, back when Chris Benoit, a wrestler Myers admired, hanged himself. Myers had said, “Oh, I’d never commit suicide. I love me way too much for that.” Then he’d grinned at her with that way he had. “Look at how pretty I am.” Now, her beautiful boy was gone.
In the car the next day, on the way to San Marcos to begin the procedural processes of death — closing up Myers’ apartment, identifying his body, speaking to investigators who had no doubt that the gunshot wound was self-inflicted — Wilbourn was on a call with the medical examiner when, out of nowhere, she heard herself asking if they could save Myers’ brain, if they could have it studied. “I just knew that the suicide didn’t make sense, because he wasn’t suicidal,” she says, her voice measured, her Texas accent melodic. “I was just praying for answers, and when the phone rang, that’s what came out. I wasn’t thinking that anything was wrong with his brain or anything like that, I just knew something wasn’t right. It’s just the mother’s instinct.”
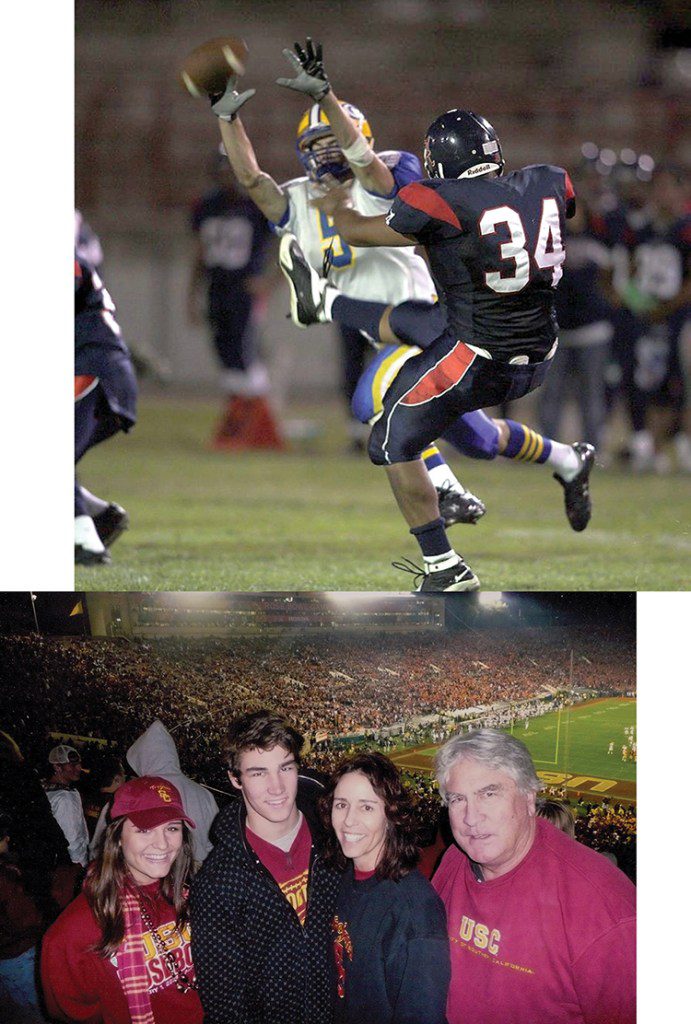
There was also, perhaps, a subconscious concern. Myers had played football for seven years, from sixth grade through his senior year of high school. In the time since he’d stopped playing, Wilbourn had learned about chronic traumatic encephalopathy — the degenerative brain disease that had plagued NFL greats like Mike Webster, Andre Waters, and Dave Duerson (who shot himself in the heart specifically so that his brain would be intact when studied). Like many people, she’d been alarmed by the reports of these famously tough athletes whose very toughness had been their undoing. Then again, she didn’t actually think Myers fit the CTE profile: He had not played football past high school; he’d never had a concussion that she knew of; he was nothing like Aaron Hernandez or Junior Seau, men who’d grown angry and addled and violent before dying angry and addled and violent deaths. So it was a surprise, she says, when “the first thing out of my mouth was ‘Can we donate his brain to Boston University?’” She looks down at the photos surrounding her. “I think that was just a God thing.”
DuQuan Myers hadn’t shown many symptoms — but was diagnosed with stage 1 CTE.
IT HAS BEEN ALMOST two decades since Pittsburgh Steelers Hall of Famer Mike Webster become the first NFL player to be diagnosed with CTE, after a heart attack at age 50 put an end to misery so intense that Webster — by then sleeping in his car because he couldn’t remember where he lived — would shoot himself with a taser gun until he mercifully blacked out. Even then, CTE wasn’t exactly a new discovery: A medical report from 1928 described boxers with “punch-drunk syndrome,” later classified as dementia pugilistica. The first known use of the term “chronic traumatic encephalopathy” occurred in a neurology paper written in 1949. But Webster’s 2005 diagnosis was a watershed moment, implicating the most popular sport in America, one grafted into the guts and glory of the American psyche — and one that millions of American kids were suiting up to play every season. So documentaries were made. Brain banks were established. Funding flowed. And as more and more brains of dead athletes were submitted for study, it became clear that, while CTE was a progressive disease, it was not the sole province of aging NFL players. It could show up in the brains of people in their teens and twenties, people who’d never played past the age of 18.
Even in CTE’s earliest stages — and for reasons scientists are still exploring — its effects could be grave. “We’re north of 1,300 brains, and while the overwhelming majority are from people who are older, we certainly have hundreds of brains of people in that younger age group,” says Dr. Robert Cantu, co-director of the Center for the Study of Traumatic Encephalopathy, chair of neurosurgery at Emerson Hospital, and the nation’s leading authority on concussions. “CTE hasn’t directly killed anybody in their teens, twenties, thirties, forties, but we have a lot of people with CTE that have died at those ages. Almost all of them have died by suicide.”
It is well-established that suffering even just one concussion is a risk factor for developing mental-health issues. The year after Myers’ death, the Journal of the American Medical Association published a study that found that a person’s risk of dying by suicide doubled after being diagnosed with a concussion. A 2021 study in the Journal of Neurotrauma followed patients for 180 days and found “significantly increased rates of depression, anxiety, or suicidal ideation following concussion” in those under 26 years of age. Another study, from 2022 and published in American Journal of Physical Medicine & Rehabilitation, found that 48 percent of all concussion patients were later diagnosed with depression, anxiety, panic disorder, post-traumatic stress disorder, bipolar disorder, or schizophrenia in the three years that they were tracked, and that “all of the mental illnesses this study chose to evaluate were present in a higher proportion of patients after a concussion than the general population.”
But CTE isn’t just about diagnosed concussions, most of which go on to heal with no obvious, lasting effects. It’s about repeated, seemingly benign assaults to brain tissue, little “dings” that could occur dozens of times in a single game and that a player may not even clock but that nonetheless cause damage at the cellular level — microscopically torn blood vessels, disconnected neurons, jumbled tau proteins (the building blocks of the fibers that carry nutrients and messages from cell to cell). Given time, the brain can usually repair this damage — except when players don’t even know there’s been damage, and so don’t grant themselves time to recover. In that case, injuries can compound until the brain is overwhelmed, until — unable to reconfigure themselves — the tau proteins essentially rot, creating toxic lesions that spread deeper into the brain and even sometimes into the brain stem. This past June, the largest CTE study to date confirmed that the best predictor of future brain disease was not the number of diagnosed concussions a player had sustained but rather the cumulative force of all hits to the head throughout their career. In other words, a lot of little impacts could be as damaging as a smattering of major ones.
This means that when kids across America suit up this fall to square off on the gridiron, every hit will matter, every “ding” and every bell rung will count toward an unspecified number past which the brain might be permanently impaired. It means that no amount of concussion protocols can definitively stave off disaster, that some level of danger is lurking in every play. It means that America’s greatest game is hurting our children in insidious and incalculable ways, and that addressing the issue might mean fundamentally changing the way we teach a game that has become fundamental to America’s sense of self.

The scars on Barrett Callaghan’s helmet were a source of pride — now, they’re a painful reminder.
Photograph by Lyndon French
“It’s a really profound problem to confront, especially for a sport that’s been at the center of so much of our community and cultural life, as youth football is and has been,” says Kathleen Bachynski, a professor of public health at Muhlenberg College and author of No Game for Boys to Play: The History of Youth Football and the Origins of a Public Health Crisis. Bachynski’s research details a long history of medical objections that have done little to intercept the sport’s cultural dominance. In the 1890s, The Chicago Tribune announced that football would “physically ruin thousands of young men.” In the early 1900s, the brutality of Ivy League games led them to be described as “boy-killing, education-prostituting, gladiatorial sport” (even Teddy Roosevelt intervened, leading to the limitation of certain plays). And throughout the 20th century, doctors continued to sound the alarm in publications like the Journal of the American Medical Association (“Football is no game for boys to play”), the Journal of School Health (“More concussions occur in football than is generally realized”), and the American Journal of Public Health (“[Children are] encouraged to addle their own brains with repeated concussions in such sports as football and boxing”). Meanwhile, as boxing declined in popularity, football’s reach only grew. Youth leagues began mushrooming in the Sixties. Kids as young as five suited up. “It’s really hard for us, societally, to confront something that we thought was great might not have been so great,” says Bachynski of this cultural expansion. “But there are some health risks that we have decided even a fully-informed parent can’t allow their kid to [take]. If you understand all the risks and harms of cigarettes, you cannot let your 12-year-old smoke a cigarette — that’s not something you can choose as a parent. And we have to decide: ‘Do repeated head impacts fall in that category?’”
For football’s defenders, the answer is no. “I love this sport. I think it’s America’s greatest sport,” says Dr. Julian Bailes, a former team physician for the Pittsburgh Steelers, a neurological consultant to the NFL Players Association, and the head of the medical advisory committee for Pop Warner, the country’s largest youth-football league. Bailes knew Mike Webster personally and, having helped identify the clinical evidence of Webster’s CTE (he’s played by Alec Baldwin in the movie Concussion), is considered to be a pioneer in the field. He certainly acknowledges the cumulative nature of the risk when it comes to head impacts and CTE, but argues that the threshold for developing the disease would be unlikely to be met just by playing a few years of youth football. “I’m not pro-head injury or pro-concussion, but there’s no conclusive evidence that if you play youth football it’s going to lead to long-term brain damage,” he tells me. “The risk occurs as [players] get into high school and college, and they are big and strong and fast and have 600 to a thousand hits a season. So in my opinion, it’s a misdirected argument. There’s probably 100 kids who get killed on bicycles every year. There’s no kids dying playing Pop Warner football.”
But science continues to raise red flags about the sport. A 2016 study published in Radiology found that playing just one season of youth football caused measurable changes in the white matter of children’s brains as well as diminished brain function, even in players who had not displayed signs of having a concussion. Another, from 2018, showed that both years of football play and the age at which an athlete started affected the volume of the thalamus, the egg-shaped structure in the center of the brain that relays information from the body and has been associated with cognition and mood. “Tau is the sexy thing to talk about, so that’s what people talk about,” says Cantu of the changes to the brain that can occur from repetitive brain injury. “They think, ‘You got CTE. That’s bad.’ Well, you can be very bad off without CTE, just from all those hits.”

Dr. Ann McKee, the chief of neuropathology at the VA Boston Healthcare System, holds slides of a brain at her lab’s brain bank in Bedford, Mass.
Shiho Fukada/The New York Times/Redux
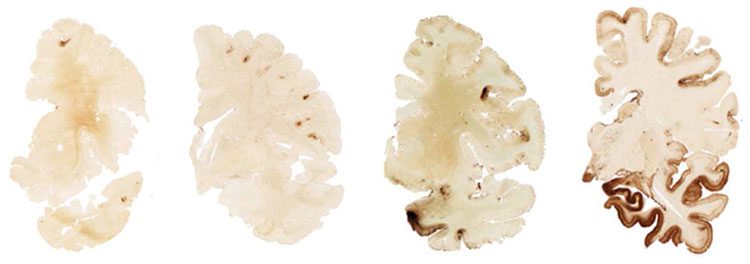
The stages of CTE, from 1 to 4. The damage at stage 1 may seem minimal but can have profound effects.
Boston University’s Chronic Traumatic Encephalopathy Center
According to Dr. Ann McKee, a neuropathologist and director of the CTE Center at Boston University — where she heads up the largest brain bank in the country — patients diagnosed with CTE almost always show other signs of brain damage, but those same injuries can still be present without the pathology of a progressive disease. “There are a lot of other changes that can cause very disabling symptoms, and they don’t have to rise to the level of CTE,” she says. “We’re seeing changes in brain architecture, shrinkage of the brain, damage to brain structures, inflammation, evidence of vascular disease — meaning the tiny blood vessels of the brain are probably injured and leaky.”
All of these changes have the potential to affect cognition and mental health. And even if the effect is difficult to quantify, with more than 2 million kids playing tackle football every year, certain researchers question whether it has led to an epidemic of children whose potential is diminished, whose cognition might have been a little higher, whose chances of developing depression or dying by suicide might have been a little lower if they had never played a sport in which they had repeatedly sustained injury to their brains. “The novel mental-health-disorder research is actually becoming quite strong,” says Chris Nowinski, a former Harvard football player and professional wrestler who went on to co-found the Concussion Legacy Foundation and get a Ph.D. in behavioral neuroscience after a concussion he suffered in the ring in 2003 kicked off a sleep disorder, a behavior disorder, and a throbbing headache that didn’t let up for years. Now considered the public face of CTE awareness — he’s the guy Newsweek called after Hernandez died by suicide in prison, and the person families typically contact if they want to donate the brain of a loved one suspected of having CTE — Nowinski not only believes that the connection between repetitive, low-level head impacts and mental illness is strong enough that developing a mood disorder could prove to be a risk factor for developing CTE, but he also believes that the connection is strong enough to be worrisome in its own right.
A study published in the Journal of Neurotrauma the month before DuQuan Myers’ death found that cumulative head impacts, with or without diagnosed concussions, increased the risk of depression, apathy, and behavioral dysregulation. A study published just a few months after his death found that participants with CTE showed accumulations of tau lesions specifically “in brain regions that have been associated with … impulsivity, depressive symptoms, anxiety, and explosivity.” Other studies have found football players to have higher rates of depression than the population at large. “Essentially,” says Nowinski, “we’re taking kids who have never had an anxiety or depression or self-harm issue, and they’re getting it because of damage to their brain.”
A MATTER OF HOURS after a bullet entered DuQuan Myers’ brain, the local medical examiner in Lockhart, Texas, carefully, gingerly, removed it and submerged it in a formaldehyde solution. She then placed the container into a styrofoam box bound for Boston. Once the brain arrived at McKee’s lab at the Boston University CTE Center, it was photographed and dissected. Half was snap-frozen and stored in perpetuity in a negative-80-degree freezer. The other half, the half that would be used to make the diagnosis, was put back in formaldehyde. Then the waiting game began.
Inside the skull of a living human, the brain is almost the consistency of jello, a miraculous mush of electrical charges. It took months for the formaldehyde to seep all the way in, hardening Myers’ brain to a consistency that would allow it to be cut into eighth-of-an-inch slivers. Those slivers were then further dissected into hundreds of 10-micron slices, almost impossibly thin ribbons of neural matter that were stained and put into slides for McKee or one of her team to analyze under a microscope. Meanwhile, clinicians were rounding up medical records to determine Myers’ medical past, his history of head impacts, and what symptoms he may have had. Both teams worked blindly: Neither would communicate about Myers’ case until the clinicians had finished their research and the pathologists had made their determination.
In the spring of 2018, Letitia Wilbourn received a notification that McKee and her colleagues had come to a conclusion in her son’s case. Not knowing what she expected or even what she wanted to hear, she arranged to take the call by herself, over her lunch break. “I didn’t want to be home alone,” she says. “I was carrying so much guilt with his suicide, thinking, ‘Did I miss something? Did I do something? What caused it?’ I had so much guilt.”
On the call, McKee gently shared the diagnosis: Myers had had stage 1 CTE, characterized by one to three microscopic lesions. At this level, the lesions would have affected such a small percentage of Myers’ brain that they may not have accounted for any changes in mood or behavior. But they would certainly have been proof of brain trauma that had been unable to fully heal. In fact, his brain also showed arteriolosclerosis (the thickening of small blood vessels), neuroinflammation, and loss of fibers in the white matter, Wilbourn was told. “Then they explained that there was nothing that I could have done to prevent what happened,” she says. “They told me that there was no way for me to have known. It was an instant release. I actually had the best day I’d had since he’d died. And then came the guilt of having put him in football to begin with.”
As gentle as he’d been off the field, Myers had been formidable on it, starting as both an offensive and defensive lineman despite his small size — only five feet five and 140 pounds by the end of high school. “He loved to tackle people, that’s for sure,” Wilbourn tells me. She thought of all those times when he had taken a brutal hit and she’d caught her breath, wondering if she should go down to the field and check on him but stopping herself with the reminder that parents weren’t supposed to do that. She thought of that time he’d broken his leg during practice and been rushed to the hospital, how she’d thought that fractured fibula and tibia were the worst injuries of his life. She thought of the terrible headaches he’d have after practices, how she’d chalked them up to allergies. She remembered how in high school he’d complained about his vision and suddenly needed glasses when no one else in the family ever had. Now, on the phone with McKee, these things took on new meaning, the past reorganizing itself in her mind.
She’d been clear with the clinicians at Boston University: Myers’ life was not without sadness. He and his girlfriend had recently broken up, though that wasn’t unusual: They’d broken up and gotten back together more times than Wilbourn could count. His cousin had just passed away, shot by an ex in an act of passion. Like the rest of the extended family, Myers had been shocked and devastated, but seemingly not any more than anyone else. On the call with Boston University, these events were referred to as “triggers,” not relevant to the official diagnosis, but certainly not irrelevant to what transpired.
“Often there’s a very impulsive component to these suicides,” McKee tells me when discussing Myers’ case this past spring. “People with an injured brain have a lower ability to control their impulses. They can be fine one minute and then all of a sudden just pull the trigger or whatever they decide to do. Their judgment is off. There’s a situation where something doesn’t go well or they become depressed, and they don’t have the checks and balances that a person who didn’t have an injured brain [would have]. We all get depressed at some point, we all feel lousy, but the injured brain just can’t stop it. They can’t pull themselves back.”
For McKee’s team, Wilbourn’s grief has become a familiar refrain. “That’s really common, in my experience, to have just a random, totally impulsive act that just blindsides the family,” McKee says. “That’s not uncommon with these suicides.”
Then again, she also has encountered plenty of cases in which the suicide is not unexpected. It’s the end that some families have been expecting, warding off, fighting back for a long, long time.
Michael Bartlett felt his brain had somehow turned on him, and he grew moody. “He knew there was something wrong,” his mom, Susan, says.
AROUND THE TIME of his freshman year of college, Michael Bartlett — the person he was, the person he’d always been — started to disappear. It happened gradually, so slowly that at first it didn’t seem like much of anything at all, maybe just a bumpy transition into adulthood. Still, his parents, Larry and Susan, grew concerned: Michael had always been friendly and easygoing, with a smile so big it seemed to hijack his entire, handsome face. On the football field, he’d been the sort of solid kid others looked up to. Now, he seemed to frustrate more easily; now, he seemed a little aloof. A year or so into these changes, Larry and Susan took him for academic testing, hoping to figure out why their smart, quizzical son — the one who’d read philosophy as a child — was struggling so much with college. The results surprised them: They were told that Michael had a very high IQ but very low cognitive function. “She said it was like having a 400 horsepower engine in a car with no wheels,” Susan says of the report. “And we’re like, ‘What does that mean?’”
What it ultimately meant was a decade of misery for her family, a decade of Michael’s brain seeming to turn on him. He tried cognitive therapy. He tried antidepressants. He tried taking medication for ADD. When none of that helped, he self-medicated with alcohol. He dropped out of college, moving home to his parents’ house in La Mesa, California, isolating himself in his room, fully aware that not just his future but something even more intangible was slipping away. “He knew there was something wrong with his brain,” says Susan. “He kept saying, ‘There’s something wrong. This is my best tool. I cannot lose my brain. I can’t.’ He tried to figure out what was wrong: ‘Maybe I have this, maybe I have that. I don’t know what’s wrong.’” She doesn’t remember him ever mentioning CTE, though the thought may have occurred to him. He’d started playing football when he was nine, coming home so beat up that Susan remembers thinking, “‘You’re not going back to that.’ That’s the stupidest thing I ever saw.” But he did go back. By his early twenties, “he started to shut down a lot. I knew we were in terrible trouble, because he would say things like, ‘If I can’t get my brain right, I can’t live.’”
Eventually, it became clear that he didn’t intend to. He got a DUI. He tried to hang himself with a belt in his closet. When Michael was arrested for lunging at the gun of one of the cops who’d responded to a suicide call, Larry couldn’t help but realize that, mixed in with the hurt and sadness, he also felt a sense of reprieve. “The thing is, he wasn’t gonna die in jail, wasn’t gonna commit suicide if he stayed there,” he says, his voice breaking. Michael never had a girlfriend. He never had a job. Larry and Susan had no idea what to do. There was no family history of mental illness, no indications of past trauma; there was only the constant vigil their life became, trying to keep their son alive. “We had problems leaving the house at all,” says Susan. “Because we were always afraid [of what we’d find] when we came home.”
When it comes to mental illness, causation is difficult, if not impossible, to prove. Many mental illnesses present in young adulthood — and their causes are certainly multifactorial. But for a number of the scientists who study CTE and brain injury, the multifactorial nature of mental illness — the nature versus nurture of it — is exactly the point. No one can predict their genetic chance of developing a mental illness; no one can predict how those odds might change after hundreds or thousands of blows to the head. “In the concussion clinic that I run, all of our clinicians doing intake evaluations ask, ‘Have you ever been diagnosed or worked up for ADD, ADHD, any learning disability, any mood disorder, anxiety, depression, panic attack?’” Cantu says. “The reason that we do this is that whenever you have an underlying challenge to start with, brain injury will only aggravate it.”
This is especially true while the brain is still developing. Though Michael Bartlett never played football past high school, he started at an age when the head is still relatively big compared with the body, and when the muscles of the neck have not been built up, meaning that even minor impacts can snap the head about. At nine, the brain is also less myelinated than it one day will be. “Myelin is the coating of nerve fibers,” Cantu explains. “It’s like the coating of a telephone wire. It not only improves transmission, but it also makes it a little harder to break, so the same degree of acceleration forces on youngsters’ brains can do more damage to the axons than they would do to an adult.”
Most importantly, according to Cantu, Bartlett began playing just before a crucial stage of brain development that, he says, occurs between the ages of 10 and 12. In these years, the circuitry is being honed — some connections between nerve cells drop out, and others are enhanced — creating the smoother neural pathways that not only allow for more efficient information processing but also dictate adult personality and intellect. “If you injure the brain during that period of time, you’re essentially causing your genetic endowment not to occur, but some aberration of it,” says Cantu. “And the aberration is not better.”
Nor is it reversible. A 2017 study on 214 former football players found that those who had started tackle football before the age of 12 were twice as likely to have “problems with behavioral regulation, apathy, and executive function” and three times more likely to have “clinically elevated depression scores,” even if they never played past high school. Another study from the following year found that participants with CTE who’d started playing tackle football before 12 developed behavioral and mood symptoms 13 years earlier than those who started at 12 or later, a pattern that was also observed in participants without CTE. (Bailes points out, however, that there are some studies that do not replicate these findings.) Younger age of first exposure to a collision sport — one in which contact doesn’t just randomly happen but is part of every play in the game — has been associated with structural alterations in the thalamus (even when adjusting for years of play) and in the corpus callosum, the bundle of nerves that connects the brain’s two hemispheres. And while damage may not become apparent until early adulthood, when cognitive demands could outpace the brain’s diminished capabilities, or may even fly under the radar — how can one measure potential that’s lost? — the bottom line, Cantu argues, is that “those who start young will have greater later-life chances to wind up with cognitive, behavioral, and mood issues — and if they get CTE, it’ll be worse.”
All of which could contribute to an explanation of what happened on July 11, 2019. Just after his 29th birthday, Michael Bartlett drove to an overpass, pulled his car over, climbed up on the concrete wall, and jumped 85 feet to the pavement below. Larry and Susan had been driving around La Mesa, frantically looking for him, when they saw the flashing red lights. “The police wouldn’t even let me see him,” Larry says. “All they would let me do is hug the body bag. I don’t even remember the next two days. It was just like we were in a different world. And it’s been that way ever since.”
These days, when Susan feels like she’s spiraling, she pulls out the report from Boston University, the one that diagnosed Michael with stage 1 CTE. “You know, when you’re in a bad place, it’s kind of helpful to see the medical answer,” she explains. It doesn’t change what happened, of course, but it achieves something: It solves the mystery Michael had been so desperate to solve when he was alive. For that, the Bartletts are grateful. “That’s where our son exists today, in Boston,” says Larry. “That’s his contribution to this horrible disease. He contributed his brain.”
THE CHICAGO SPRING RECEPTION hosted by the Concussion Legacy Foundation is a cascade of grief amid canapes. One evening this past spring, in a lovely room of the University Club with sweeping views of downtown, family members of the deceased or desperate stand up one by one to share their plight. There is the young son who speaks of his father’s decline, the dad who wants to honor his child’s memory, the teammate who wonders if his friend’s struggles await him also. Toward the end of the impromptu speeches, Jan Callaghan falteringly makes her way to the center of the room. Her son Barrett’s legacy story is on the CLF’s website, alongside a photo of the football helmet he’d worn in middle school, the one scarred with deep gashes and gouges.
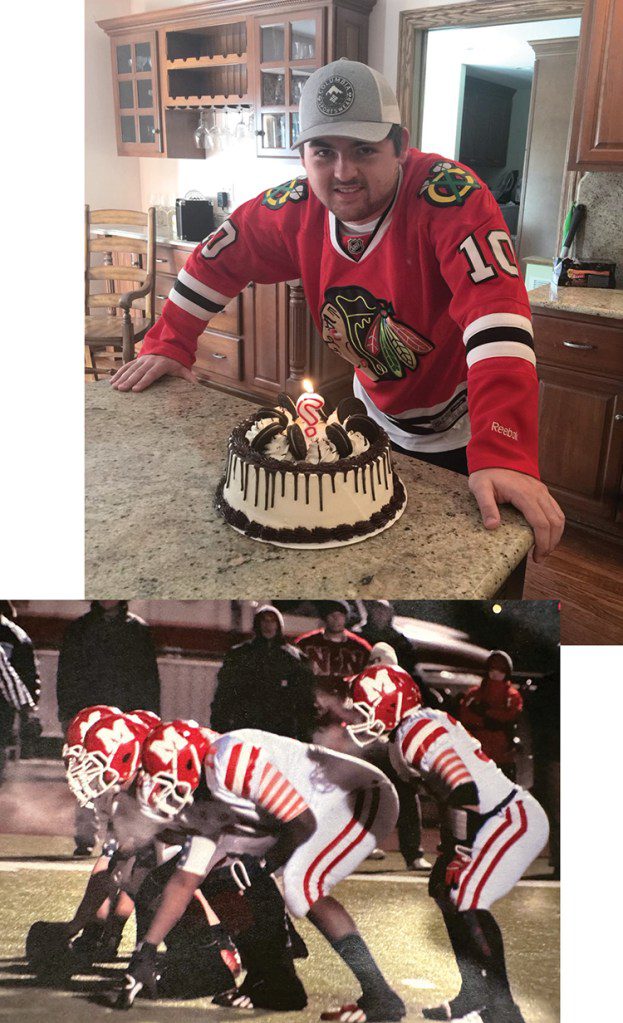
After high school, Barrett Callaghan lived in a daze. His parents later learned he had stage 1 CTE.
She’d pointed them out the day before, standing over the helmet as it rested on the dining-room table of her house in the Orland Park neighborhood of Chicago. There was a time when those gouges were a source of pride. Now, Jan shudders at the thought.
For years, hers had been a football family, their lives arranged around the endless drills and practices, their weekends spent driving to and from games, their laundry hamper full of grass-stained uniforms. When he was seven, Barrett saw his brother Richie play and begged his parents to find a team for him. Jan remembers getting a call from her husband during one of Barrett’s first games: “He said, ‘You’ve got to get up here. You’re not going to believe this.’” As she approached the field, she searched out Barrett’s little red uniform with the number 3. “And my jaw dropped as I watched him go from one end of the field to the other with the football, never stopping. As a young boy, he was a force. When that football hit his hands, there was no stopping him.”
As Barrett got older, it became clear that he’d never play professionally, but it was also clear that football would organize the rhythms of his life. One of his sisters was a cheerleader. His dad, Rich, volunteered as a coach. “The slogan we had was ‘Don’t drop your bonnet,’” he says the day we meet, sitting at the kitchen table, his voice thick with sorrow. “‘Tackle the right way, into the chest with your face guard up. Don’t have your head down.’” Richie had heeded this warning. But Barrett was a different sort of player than his brother, one who made up for his small size with his tenacity. “He was a really tough player,” Jan says. “He did play with his head.”
There were a lot of tough players on the South Side of Chicago, where the kids attended Catholic school and where football came second to God, if only just. “They call it the black-and-blue South Side Catholic,” says Rich. “Because the kids are black and blue.” So it was hard to explain to football friends what was happening to Barrett in the final years of his life. People thought he was lazy when he dropped out of college and moved back home, unfocused when he couldn’t hold down a job, losing the thread when he’d lash out aggressively for almost no reason. People distanced themselves. Jan would have to remind them, “This is Barrett we’re talking about. You’ve known him forever. Do you think it was normal that he couldn’t finish school?” She saw how he couldn’t sleep, how embarrassed he was when he couldn’t take in simple information or remember simple tasks, how he saw his brother and sisters building lives and careers and families and felt desperately left behind. When he came down to the kitchen one summer afternoon and told Jan he thought he had CTE, she had already come to the same conclusion. She assumed she’d go the rest of her life not knowing for sure. But when state troopers knocked on her door at 4 a.m. the morning of Sept. 26, 2021, and told her that Barrett had died in an accident, a head-on collision with a car going the wrong way on the highway, she had barely been able to even take in the news before she started making plans to have his brain donated.
As with smoking and lung cancer, there’s no known threshold for developing CTE and no way to know an individual player’s risk factors for being affected by it or other structural changes to the brain — no way to yet explain why some players are ravaged while others seemingly escape harm. On average, those who play a collision sport for less than five years have a very small chance of getting diagnosed with the disease, but the risk goes up after that; at 15 years of play, the risk has been estimated to be 10 times higher. The location of the damage probably matters, too; some parts of the brain are “silent” and harm to them could pass unnoticed, while others are crucial to cognition and regulation of mood. And some people may just take longer to heal, making them more susceptible to outrunning their cognitive reserve. “Probably in some cases, the brain’s regulatory systems are not very good — they are more fragile — so the brain cannot bring itself back to normality,” says Dr. Lea Grinberg, a neuropathologist who studies the early stages of neurodegenerative disease and whose 2018 study on Alzheimer’s found it to also be preceded by mood dysregulation.
Despite these unknowns, the diagnosis of stage 1 CTE has been enlightening, but further isolating for Barrett’s family. “This woman whose husband took his life brought up this great point,” Jan tells me. “She said, ‘Everybody went on and on when he passed about what a hard, tough player he was and a great teammate. And then when I told everybody that he had CTE? Crickets. Nobody wants to talk about it.’” She looks down at her hands spread over the table. “It’s like you’re on an island,” she continues. “I don’t know if they just don’t believe it, or they don’t want their precious little football tarnished.” Or maybe, she considers, they just don’t want to have to face the possibility that the same fate could await their kid, which is a reservation she understands.
Even Rich had trouble accepting Barrett’s diagnosis at first, though time and research have helped him come around. “There’s clearly more than a smoking gun here,” he says. “The gun’s been fired.” Jan nods in agreement: “You pay attention, or you don’t.”
IN RECENT YEARS, plenty of people have paid attention. According to the Sports and Fitness Industry Association, participation in tackle football for kids ages six to 12 has declined almost 29 percent since 2016, the year the NFL first publicly (and belatedly) confirmed a link between football and CTE — which has now also been found in the brains of hockey, soccer, and rugby players, as well as wrestlers, mixed-martial artists, and the first woman, Australian rules footballer Heather Anderson, who died last year at the age of 28 by an apparent suicide. Meanwhile, every state in the nation has passed laws aimed at protecting children who get concussions playing sports, and helmets have undergone overhauls in pursuit of the perfect padding. U.S.A. Football, which governs the amateur arm of the sport, has promoted “heads up” tackling and concussion training. Pop Warner introduced concussion guidelines in 2010 (including the mandate that anyone suspected of having a concussion must be cleared by a medical professional), banned full-speed head-on blocking and tackling drills in 2012, limited full-contact practices to 25 percent of the time and banned kickoffs (the game’s most dangerous play) for athletes under the age of 11 in 2016, and got rid of the three-point stance (which lowers a player’s head) in its younger divisions in 2019. (Changes have also been made to youth hockey and soccer.)
Yet many brain scientists and public-health officials question whether some of these changes are having a demonstrable effect, or even an effect at all, when it comes to the most insidious forms of brain injury. Many states’ laws tend to deal with managing concussions after they happen, not preventing them. When it comes to helmets, improvements better protect the skull, but they do not stop the brain from ricocheting inside of it, slamming against bone, torquing the brain stem; in fact, the more padding a helmet has — and thus the heavier it is — the more of a weapon it ostensibly becomes. A British Journal of Sports Medicine study from 2017 found that new protective equipment had no measurable effect on concussion prevention, much less on the prevention of non- or subconcussive blows. Leagues that use heads-up techniques have actually recorded slightly more concussions (though the increase was statistically insignificant).
According to Cantu and Nowinski, the only changes that demonstrably help are those that reduce contact overall, like the ones Pop Warner has implemented in the face of declining participation. Yet such changes are only as good as their enforcement, and while volunteer coaches may mean well — and may no longer subscribe to the myth that their job is to turn grade-schoolers into gladiators — they may also take false comfort in pronouncements that attempt to undermine the connection between CTE and collision sports and that are sometimes made by organizations with a financial stake in keeping that connection blurry. The International Consensus Conference on Concussion in Sport, an entity responsible for issuing the guidance that informs sports protocols across the globe — and one led by a number of scientists with ties to sports organizations — has consistently published statements that treat the science as unsettled, providing legal cover to conference sponsors like FIFA and World Rugby should they be accused of covering up known risks. In 2016, Pop Warner settled a case brought by the mother of a former player who died by suicide at age 25 and was later found to have CTE, opening the door to other potential lawsuits. (“At Pop Warner, there is nothing more important than the safety of our players, and since 2010, we have led the way in making the game of youth football a safer and better experience than ever before,” the organization stated in response to the settlement.)
For whatever reason, there are certainly scientists who tend to focus not on what’s known — that exposure to collision sports is the one constant in nearly all documented cases of CTE and that CTE is not the only negative neural outcome — but instead on what’s unknown. “Nobody’s looking at chess players to see if they die by CTE,” says Dr. Michael Lewis, who specializes in preventive medicine and serves on the Pop Warner Youth Football Medical Advisory Board. While Lewis supports the changes Pop Warner has made, he also argues that they are solutions to a problem that may be overstated — or oversimplified by pointing a finger at collision sports. “I mean, I kind of look at it as the climate-change thing. Is the science settled on climate change? I don’t think so. But what’s the downside of cutting back on carbons? [When it comes to] getting your head hit or whatever, there’s no downside to decreasing the exposures. We kind of look at it as, ‘OK, the science is anywhere but settled, but let’s be conservative and let’s limit the amount of contact in practice.’ Let me just say, it’s not straightforward. It’s the brain. It’s complicated.”
Such a stance puts one of the doctors advising the nation’s largest youth-football organization behind not just the NIH but even the NFL in acknowledging the connection between football and CTE. But one need look no further than the American Academy of Pediatrics to see the sway football has had over science. In 1957, the academy advised against collision sports for children ages 12 and younger, concluding that “body-contact sports, particularly tackle football and boxing, are considered to have no place in programs for children [of this age].” Since that time, and even as an abundance of evidence of brain trauma has come to light, the academy’s stance has softened. In 2015, the AAP — the same group that recommends against body-checking in hockey in players under the age of 15 due to concussion risk — released a policy statement that essentially sidestepped the issue when it comes to America’s most popular game. It conceded that eliminating youth tackle football would “likely lead to a decrease in the incidence of overall injuries, severe injuries, catastrophic injuries, and concussions,” but also argued that it would “lead to a fundamental change in the way the game is played.”
In light of this trade-off, the AAP, the agency tasked with advising parents and pediatricians about reasonable risk, essentially passed the responsibility for that determination on to them: “Participants in football must decide whether the potential health risks of sustaining these injuries are outweighed by the recreational benefits associated with proper tackling.” (When approached about this policy, a representative from the AAP informed Rolling Stone that it was “currently undergoing an update.”)
Thus far, CTE can only be diagnosed postmortem, though this month, Bailes’ research team will begin stage three of an FDA trial to diagnose the disease in living people using PET scans and MRIs. This would be a significant breakthrough, not just enabling those with the disease to get early intervention but also allowing for the possibility of treatment. “There’s plenty of potential treatments,” says McKee. “But it’s hard to assess their efficacy without having a biomarker to follow to see if it’s getting better. That’s part of the problem right now: We can’t diagnose it during life, so we can’t follow a treatment to see if it’s actually beneficial. But I think we’re going to get there.”
Until then — and in light of not just CTE but other potential cognitive and mental-health outcomes — many doctors and scientists argue that the best approach from a public-health perspective is to outlaw the collision part of collision sports, at least until children’s brains have passed the period of rapid development in their tween years. The Concussion Legacy Foundation’s “Stop Hitting Kids in the Head” campaign has encouraged parents to hold off on enrolling their kids in tackle football until they are 14. Cantu has called on the surgeon general to ban tackle football for children under that age, pointing out that all of the health and social benefits of a team sport can be retained in less-violent versions of these games (in fact, the Manning brothers famously didn’t start playing tackle football until middle school). McKee goes even further, arguing that no one should play a collision sport until they reach the age of consent, until they are emotionally mature enough to weigh the risks themselves and physically mature enough to better withstand them. That may sound extreme to football diehards, but not to McKee, who spends her days looking at damaged brains and speaking to the devastated families who donate them. “Part of the reason I can’t let this go is I know what it’s doing to people,” she tells me. “And I also know it’s preventable.”
A TEXAS THUNDERSTORM is brewing, the air growing hot and thick with the smell of the coming rain, on the recent Saturday morning when Letitia Wilbourn visits her son’s grave. Under the shade of the oak tree where the doves once perched, she rearranges the plastic flowers and carefully sweeps dust off the gravestone with a little brush she keeps in the car for that purpose. Her daughter Natasha stands there and cries. Wilbourn tries to keep herself busy. “I promised Quan I wouldn’t break,” she says, walking back to her car. “I told him I will always try to smile when I’m discussing him.”
Back home, Wilbourn sits on the floor of her living room, in view of Myers’ football trophies, surrounded by his photos, down the hall from the room where his clothes still hang in the closet. The extended family has gathered today, assorted cousins, aunts, uncles, and grandchildren passing through the room and in and out of the house, a tight-knit, boisterous group of which Wilbourn seems to be the calm and stoic center. Life goes on, certainly, even if, in some ways, it now revolves around the memory of death. “If Quan was still here right now, then he probably would be dealing with something mentally in his head,” Natasha offers haltingly. “Like, how would he be today? Would he be outside walking around with his shirt off? No shoes? Where would he be?”
Wilbourn’s oldest child, Monique, nods. They all know the CTE narrative, the tragic way it unfolds. “What would have been the progression? Would we have to have been looking for him out in the streets?”
“I don’t know if I would be happy seeing him here right now with dementia versus what happened,” Natasha says, beginning to cry again. Wilbourn reaches for her daughter’s hand. Still, she doesn’t break.
There are times when she does. Sometimes, she’ll be driving and pass a field with peewee players huddled together, their little helmets and bodies clashing under the Texas sun, and she won’t be able to look away. “I pull over and pray for every kid out there,” she tells me. “I pray, and I cry.” When people ask about her son, she tells them about CTE. She implores parents to consider other sports. She wants her son’s death — her own suffering — to have some purpose, some meaning. But, she tells me, “this is Texas, and football is God to some people.”
As we’re talking, a 12-year-old boy walks into the room and sits silently on the sofa. He’s Wilbourn’s nephew’s child. He started playing tackle football this past year, despite his family’s experience with CTE, despite Wilbourn’s admonishments, despite the fact that his father sits nervously on the sideline of each game, watching his son’s head and the movements of his body, looking for signs of disaster. This very afternoon, the boy is a witness to his family’s grief, yet it won’t stop him from playing this game of neural Russian roulette. What can Wilbourn do? He isn’t her child. All she can do is pray that maybe, just maybe, this is a game he’ll win.